

Communication gaps between clinical and non-clinical staff
In most hospitals, communication gaps between clinical and non-clinical staff exist because clinical and non-clinical staff inhabit parallel worlds with separate vocabularies, different time horizons, and fundamentally different assumptions about whose job it is to communicate.
The result is a persistent information gap that affects patient care, operational efficiency, and the engagement of every person caught on either side of it. This article names the mechanisms behind this gap, the Status Gap Model, information asymmetry, and the 5 failure modes, and provides a bridging framework for hospital operations teams.


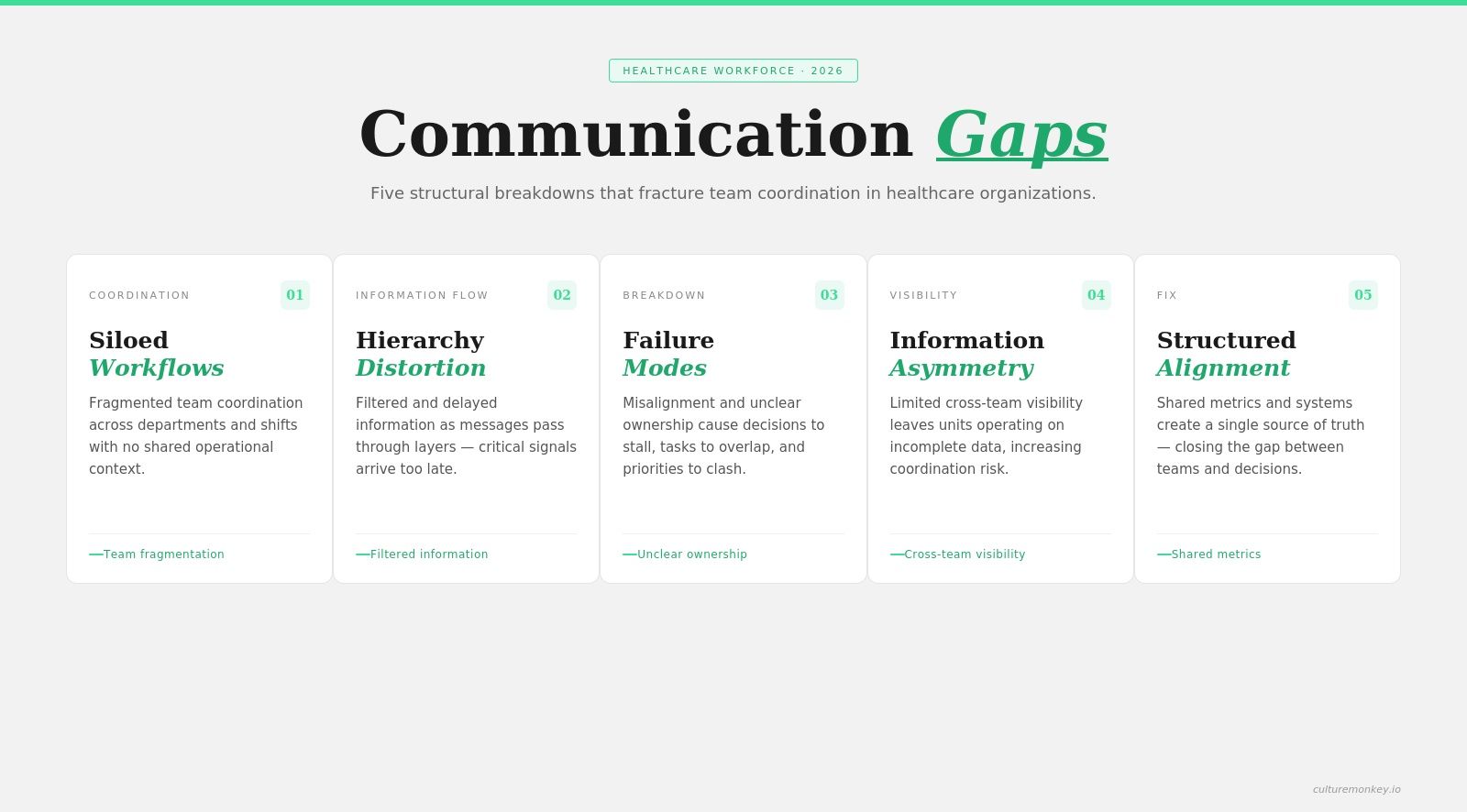
- Clinical and non-clinical staff operate in silos, creating fragmented workflows and misaligned communication priorities across hospital systems.
- Hierarchy distorts communication flow, causing filtered information, delayed escalation, and reduced clarity between decision-makers and operational teams.
- Five recurring failure modes drive breakdowns, including misaligned goals, unclear ownership, delayed feedback, fragmented tools, and assumptions.
- Information asymmetry limits visibility, where non-clinical teams lack context, and clinical teams lack operational transparency for decisions.
- Closing communication gaps requires structured mechanisms, shared metrics, and continuous measurement of communication health across hospital teams.
Why clinical and non-clinical staff exist in separate communication worlds

In hospitals, the clinical-non-clinical communication gap exists because teams operate with different priorities, language, and accountability structures.
Healthcare professionals focus on patient outcomes, while healthcare providers in administrative roles manage processes, creating misalignment in how information is shared, interpreted, and acted on across daily operations.
- Different training cultures: clinical training emphasises rapid decisions under uncertainty, while non-clinical teams optimise processes and compliance, creating a clinical-non-clinical communication hospital divide where effective communication breaks down due to mismatched mental models and expectations.
- Conflicting time horizons: clinicians operate in minutes and outcomes, while administrative teams think in weeks, budgets, and planning cycles, leading to misaligned communication strategies where urgency is either overestimated or under-responded across healthcare professionals and providers.
- Unequal authority signals: clinical voices often carry decision weight in patient care, while non-clinical input is seen as support, distorting effective communication and limiting cross-functional influence in hospital operations and system-level decisions.
- Language and vocabulary gaps: clinical terminology and operational language rarely overlap, causing interpretation errors where healthcare providers and support teams misunderstand intent, slowing coordination and reinforcing the clinical non-clinical communication gap across daily workflows.
- Ownership ambiguity: both sides assume the other is responsible for updates and coordination, weakening communication strategies and creating delays, missed handoffs, and friction points that impact effective communication across hospital teams.
- Tool and workflow fragmentation: clinical systems and administrative platforms often do not integrate, forcing healthcare professionals and non-clinical teams into parallel workflows, which reduces visibility and prevents effective communication across shared processes.
The status gap model: How hierarchy distorts information flow.
A hospital hierarchy is like a filter that changes what each role can see, question, or escalate. In status gap hospital communication, authority shapes whose updates travel fast, whose concerns get softened, and whose input is delayed, creating poor communication patterns that weaken coordination across healthcare teams and affect patient care.
- Information follows rank: in doctor support staff communication, updates often move upward only after being filtered, simplified, or delayed, which leaves healthcare teams working with partial context and increases poor communication risks that can affect patient care, patient safety, and decision speed.
- Concerns are softened before escalation: lower-status staff may reword risks to sound less confrontational, which hides urgency from healthcare leaders and the care team, increasing the chance of medical errors and serious medical errors when action depends on clear, timely communication.
- Clinical authority shapes response time: when the same issue is raised by different roles, senior clinical voices often receive faster attention, creating a status gap in hospital communication where valid operational concerns from support staff reach decision-makers late and affect patient outcomes.

Improving communication is one of the most effective ways to improve patient outcomes.

- Support roles get information in fragments: non-clinical teams often receive instructions without full clinical reasoning, making execution harder across healthcare organisations and increasing poor communication between functions, especially when staff must coordinate scheduling, discharge planning, transport, documentation, and service recovery.
- Frontline observations lose weight: support staff and junior employees often notice workflow risks early, but weak doctor support staff communication can keep those signals from influencing the care team, limiting chances for improving patient safety and achieving better patient outcomes.
- Hierarchy discourages clarification: when staff feel they should not question senior voices, structured communication tools become essential because silence, hesitation, and assumed understanding can create avoidable gaps that contribute to medical errors, patient safety failures, and uneven patient care.
- Form matters as much as timing: hierarchy influences not just when information is shared, but how it is framed, who is copied, and what gets emphasised, which is why healthcare leaders need structured communication tools to reduce distortion across healthcare teams.
The 5 communication failure modes across the clinical/non-clinical divide

Hospital communication breakdowns across the clinical-non-clinical divide reflect a broader interprofessional communication failure healthcare issue, where intent, urgency, and visibility are misaligned between teams. Information is shared, but meaning is lost or misinterpreted, creating coordination gaps that affect workflows, slow decisions, and impact patient care across departments.
1. Clinical jargon exclusion
Clinical teams often use specialised language that non-clinical staff cannot fully interpret, creating hospital communication breakdowns where instructions are followed without clarity, increasing errors, delays, and rework across the clinical-non-clinical divide in routine operations.
2. Priority-perception mismatch
Clinicians prioritise patient urgency while non-clinical teams balance schedules and systems, leading to conflicting interpretations of what matters most, which reinforces the clinical-non-clinical divide and causes missed deadlines, friction, and inconsistent execution across hospital workflows.
3. Information hoarding
Critical updates are sometimes held within teams due to ownership boundaries or assumptions, creating hospital communication breakdowns where downstream teams lack visibility, slowing decisions, and increasing coordination gaps across the clinical-non-clinical divide.
4. Handover invisibility
Transitions between teams often lack structured communication, making key details invisible to the next team, which results in repeated follow-ups, missed context, and inefficiencies that deepen the clinical-non-clinical divide across patient and operational handovers.
5. Recognition asymmetry
Clinical contributions are often more visible than support roles, leading to disengagement and reduced initiative from non-clinical staff, which weakens collaboration and sustains hospital communication breakdowns across the clinical-non-clinical divide.
Information asymmetry in hospital operations
Hospital information asymmetry occurs when clinical teams hold patient-critical details that operational teams need, but systems fail to transfer them fully. This leads to interdepartmental communication failure across healthcare settings, where teams act without enough context, affecting coordination, response time, and the ability to communicate effectively.
- Patient context stays with clinical teams: operational staff often receive tasks without the full picture of a patient's condition, which creates hospital interdepartmental communication problems during scheduling, discharge planning, transport, and bed management, especially when communication tools do not carry the clinical context behind each request.
- Patient transfers expose the gap quickly: during patient transfers, non-clinical teams may know where a patient is going but not why urgency has changed, which increases communication failures, slows coordination, and creates nurse admin communication breakdown when teams must respond without enough context or shared visibility.
- The emergency department amplifies delays: in the emergency department, rapid changes in patient status require support teams to adjust quickly, but interdepartmental communication failure occurs when updates stay inside clinical channels, causing avoidable delays in transport, admissions, environmental readiness, and downstream operational planning.
- Operational decisions get made half-informed: support teams are expected to improve communication and execution, yet they often act on partial instructions, which raises the risk of medical mistakes, weakens patient handoffs, and creates frustration when each team member is judged on outcomes they were not equipped to influence.
(Source: Gallup)
- Communication tools do not transfer meaning: many communication tools move messages between departments, but they do not always explain priority, dependency, or risk, making it harder to communicate effectively across healthcare settings and increasing hospital interdepartmental communication problems during time-sensitive workflows and shared service coordination.
- The patient experience absorbs the fallout: when non-clinical teams lack timely context, delays become visible to patients through repeated questions, inconsistent updates, and missed expectations, which healthcare research increasingly links to communication failures, weaker trust, and poorer patient experience across the full care journey.
- Asymmetry weakens shared accountability: when one side holds the context, and the other carries the task, ownership becomes uneven, which makes it harder for teams to improve communication, fix root causes, and prevent the same nurse admin communication breakdown from repeating across departments.
How communication gaps affect engagement on both sides

Communication gaps in engagement with hospital issues reflect a broader hospital silo communication problem affecting trust, workload, and visibility. When information exchange fails, non-clinical disengagement rises while clinical staff absorb coordination work, weakening ownership, situational awareness, and collaboration. Communication failures contribute to 30% of malpractice claims, resulting in 1,744 deaths and $1.7 billion in costs, showing how these gaps directly impact patient safety.
The bridging framework: 5 mechanisms that close the gap
To improve clinical and non-clinical communication, hospitals need consistent mechanisms that connect clinical staff and support teams. Clear movement of patient information reduces adverse events, supports optimal care, and improves coordination across health care operations through structured, repeatable communication practices.
1. Shared briefings
Structured, recurring briefings align clinical staff and hospital staff on patient information, priorities, and risks, enabling open communication, fewer interruptions during execution, and clearer coordination that supports optimal care while reducing adverse events across health care workflows.
2. Liaison roles
Designated staff members translate between clinical and non-clinical teams, ensuring patient information, including family history and care dependencies, is understood in their own words, improving medical care coordination and reducing gaps that can lead to malpractice costs.
3. Cross-functional huddles
Short, focused huddles create space for active listening, where hospital staff and clinical staff clarify updates, resolve blockers, and align next steps, strengthening open communication and reducing delays, confusion, and breakdowns in fast-moving health care environments.
4. Common language protocols
Standardised formats help staff members communicate priorities clearly without jargon, making patient information easier to act on, improving medical care execution, and reducing the risk of adverse events caused by misinterpretation across teams.
5. Information handover standards
Consistent templates ensure patient information moves completely and accurately between teams, reducing missed details, limiting malpractice costs, and supporting optimal care by giving every team shared visibility at critical transition points.
measuring clinical/non-clinical communication health.
Hospital communication measurement helps identify where communication works and where it breaks across teams. An interdepartmental survey and audit framework shows whether nurses, clinicians, and operational staff communicate clearly, share important information reliably, and stay aligned across shift changes, workflows, and responsibilities.
- Use survey items tied to real work: ask whether team members receive important information on time, know who is responsible, and can communicate clearly across departments. This makes hospital communication measurement useful inside a hospital because it captures daily friction, not vague opinions.
- Measure clarity during handoffs and shift changes: test whether nurses, clinicians, and support teams understand updates during shift changes, patient movement, and service coordination. When teams fall short here, patients face delays, rework grows, and communication failures create a negative effect across the full team.
- Audit where messages lose meaning: track where more messages are being sent, but less understanding is created. In many healthcare environments, volume hides weak communication, so leaders need an example-based audit that shows where teams communicate often, yet still miss context, ownership, or timing.
- Check cross-department trust and response quality: measure whether people feel heard, whether follow-ups happen, and whether other departments act on shared updates. This shows whether communication strategies are working in practice or whether teams still fall short when pressure rises across hospital operations.
- Look for role-based differences in experience: compare responses from clinicians, nurses, and non-clinical staff to find gaps in visibility, timing, and accountability. This helps healthcare leaders see whether one group consistently receives less context or carries more coordination work than others.
- Link communication data to safety and service risks: use findings to review delays, repeated escalations, complaints, and missed updates involving patients. Joint Commission expectations make this practical, because communication quality is not just cultural; it affects whether hospitals transfer important information reliably.
Conclusion
Communication gaps between clinical and non-clinical staff directly affect treatment quality, operational practice, and overall workplace trust. When these gaps persist, they increase risk, delay decisions, and reduce how effectively each person contributes to patient care. Addressing this requires structured listening, clear accountability, and consistent communication systems.
CultureMonkey helps healthcare organisations bridge these gaps by capturing real-time feedback, identifying breakdowns, and enabling teams to act on insights with the right resources. By improving visibility and coordination, it supports stronger collaboration, reduces risk, and builds a workplace where every person can contribute effectively to better outcomes.
FAQs
1. Why do clinical and non-clinical staff struggle to communicate?
Three structural mechanisms drive the gap: the status gap (clinical authority determines information access), information asymmetry (patient-critical data sits with clinical teams but isn't transferred operationally), and cultural divergence (clinical training emphasises precision; operational training emphasises efficiency), creating stress across shifts and weakening collaboration between physicians, doctors, and operational teams.
2. What is the status gap in hospital communication?
The status gap describes how professional hierarchy determines not just decision authority but information access. Physicians and doctors receive information first and in full detail. Non-clinical staff receive filtered, delayed, or no information, not from malice, but from a system that wasn't designed to include them, especially across shift-based coordination.
3. How does poor interdepartmental communication affect patient care?
When teams fail to collaborate effectively, patient discharges are delayed by facilities bottlenecks, equipment failures go unreported, supply shortages surprise doctors and physicians, and administrative errors compound in records, increasing stress across shifts and raising patient risk significantly.
4. What causes communication silos in hospitals?
Communication silos form due to hierarchy-driven access, fragmented systems, and role-based workflows. Clinical and operational teams use different tools, languages, and priorities, which limits information flow, reduces visibility, and prevents consistent collaboration across departments, especially during shift changes and cross-functional coordination.
5. How do communication gaps between clinical and non-clinical staff affect hospital efficiency?
Communication gaps slow coordination by delaying decisions, duplicating work, and increasing follow-ups across departments. When teams lack shared visibility, processes like discharge, transport, and scheduling break down. This reduces efficiency, increases workload pressure, and creates avoidable delays that impact both patient flow and staff productivity.
6. What are the most common communication failure modes in hospitals?
Common failure modes include jargon exclusion, priority mismatch, information hoarding, handover invisibility, and recognition asymmetry. These patterns create repeated breakdowns where intent is misunderstood, urgency is misaligned, and key details are missed, leading to coordination gaps across clinical and non-clinical teams.
7. How can hospitals improve communication between clinical and non-clinical teams?
Hospitals can improve communication by introducing shared briefings, cross-functional huddles, liaison roles, standardised language protocols, and structured handover processes. These mechanisms ensure information flows clearly, reduce misinterpretation, and help teams align on priorities, improving coordination and reducing errors across departments.
8. What metrics should hospitals track to measure communication effectiveness?
Hospitals should track clarity of handoffs, timeliness of information sharing, cross-team response rates, and alignment during shift changes. Survey-based feedback from clinicians and support staff can reveal gaps in visibility and coordination, helping leaders identify where communication breaks down and needs improvement.






{kind=link}