

Building a feedback culture in healthcare institutions in 2026
Building a feedback culture in healthcare institutions creates conditions where staff consistently share honest, actionable feedback without fear. It is reflected in whether people speak up in real clinical situations, and not just in the presence of healthcare survey tools.
This guide is based on tested frameworks designed for healthcare institutions. It shows how to enable employee voice, reduce silence, and build systems where constructive feedback leads to visible, trusted action.


- Building a feedback culture in healthcare means enabling staff to share honest, actionable input without fear of hierarchy or retaliation.
- Clinical silence stems from hierarchy intimidation, retaliation risk, perceived futility, and doubts about anonymity in small teams.
- Anonymous feedback in small teams needs controls like aggregation, external facilitation, and batched reporting.
- Visible action on feedback sustains participation, as without follow-through, feedback cultures lose trust and engagement.
- CultureMonkey builds feedback culture in healthcare institutions through anonymity thresholds, multi-channel collection, and real-time dashboards.
What is a feedback culture in healthcare institutions?
A feedback culture in healthcare institutions is defined by the conditions under which staff feel safe to give honest, specific, and actionable input. It is not about surveys or tools, but whether people consistently don't hesitate in delivering feedback when it matters.
A true culture of feedback supports both professional development and personal development across roles. It ensures open communication between teams, improving both collaboration and patient care outcomes.
This means positive and negative feedback culture is measured by behavior, not infrastructure:
- Do nurses escalate concerns early?
- Do junior staff question decisions safely?
- Do teams report issues without fear?
These behaviors reflect whether healthcare workers operate in a supportive environment or a restrictive one.
If staff choose silence over input, the feedback culture in the healthcare environment is not functioning, regardless of how many tools are in place.

Employee engagement is the emotional commitment the employee has to the organization and its goals.
Kevin Kruse

![]()
Founder and CEO at TalentCulture
Why do clinical staff fear giving feedback?
Clinical staff fear giving feedback due to hierarchy, retaliation risk, perceived futility, and lack of anonymity. These speaking up culture barriers make feedback delivered feel unsafe or ineffective.
1. Hierarchy fear
Hierarchy fear occurs when clinical staff avoid giving feedback because healthcare structures prioritize authority over open dialogue. Junior staff often withhold concerns to avoid challenging senior decision-making.
2. Retaliation risk
Retaliation risk arises when staff believe non-positive feedback could lead to negative consequences such as poor evaluations, shift changes, or career impact. Even perceived risk is enough to suppress honest input.
3. Perceived futility
Perceived futility occurs when clinical staff believe their feedback will not lead to change. When previous input has been ignored, staff disengage from giving feedback altogether.
4. Anonymity doubt in small teams
Anonymity doubt in small teams occurs when staff believe their identity can be inferred despite anonymous systems. This reduces trust and limits honest, formal and informal feedback in tightly knit clinical units.
Anonymous vs. named feedback in clinical settings: When to use each
Use anonymous feedback when staff face risk, power distance, or sensitive issues, and use named feedback when trust exists and follow-up or accountability is required. In clinical settings, anonymity protects honesty in high-risk environments, while named feedback enables direct action, clarification, and ownership of outcomes.
What is the psychological safety hierarchy in healthcare settings?
The psychological safety hierarchy for healthcare settings is a five-level progression from physical safety to organizational trust. Each level determines whether staff will speak up, challenge decisions, and contribute honest feedback in a psychological safety hospital environment. Most healthcare feedback cultures fail at Level 3 (voice safety) because hierarchy and retaliation risk block staff from sharing input without fear of consequences.
This clinical psychological safety model includes five levels:
Level 1: Physical safety
Physical safety ensures staff can work without risk of harm from the environment, workload, or unsafe conditions. Without this baseline, higher levels of psychological safety cannot exist.
Level 2: Identity safety
Identity safety ensures staff are respected regardless of role, background, or experience. When identity is sensed to be threatened, staff avoid visibility and withhold input.
Level 3: Voice safety
Voice safety exists when staff can share concerns, report risks, and give feedback without fear of negative consequences. This is where most feedback cultures fail.
Level 4: Challenge safety
Challenge safety allows staff to question decisions, challenge authority, and suggest alternatives. It reflects whether hierarchy can be safely navigated.
Level 5: Organizational trust
Organizational trust exists when staff believe the feedback process will lead to fair action and meaningful change. Without trust, speaking up feels pointless.
Formal vs. informal feedback in healthcare institutions
Use formal feedback for structured, documented input that informs decisions, and informal feedback for real-time, low-stakes conversations during daily work. In healthcare institutions, formal feedback ensures consistency and accountability, while informal feedback enables immediate course correction and continuous improvement.
How does the hospital hierarchy suppress honest feedback?
In hospital hierarchy feedback suppression, the consultant-to-nurse dynamic makes upward feedback feel risky, inappropriate, or futile. The consultant-to-nurse dynamic often discourages input upward, even when risks are visible.
1. Authority gradient normalizes silence
In clinical hierarchies, consultants make decisions and nurses execute them. This structure signals that questioning decisions is not expected, so staff withhold concerns even when risks are visible.
2. Feedback is perceived as challenge, not input
Upward feedback is often interpreted as questioning competence or authority. This reframes effective feedback as conflict, causing staff to filter or soften critical information.
3. Career and relationship risk outweigh the benefit
Staff assess the personal cost of speaking up against uncertain outcomes. When the risk to evaluations, shifts, or relationships is high, silence becomes the safer choice.
4. Clinical governance feedback exists, but is bypassed
Formal clinical governance feedback systems may exist, but real-time, effective feedback is avoided. Staff rely on delayed reporting instead of immediate escalation.
Interventions that interrupt hierarchy-driven suppression
5. Normalize upward feedback in critical moments
Embed structured prompts where junior staff must share concerns during decision-making points. This shifts feedback from optional to expected.
6. Redefine feedback as patient safety input
Position effective feedback as a safety requirement, not a personal challenge. This reduces defensiveness in senior roles.
7. Make leader's response visible and consistent
Senior clinicians must acknowledge and act on feedback in real time, while also helping to improve patient outcomes. Consistent response behavior weakens hierarchy-driven silence over time.
How do clinical leaders build and sustain a feedback culture in healthcare?
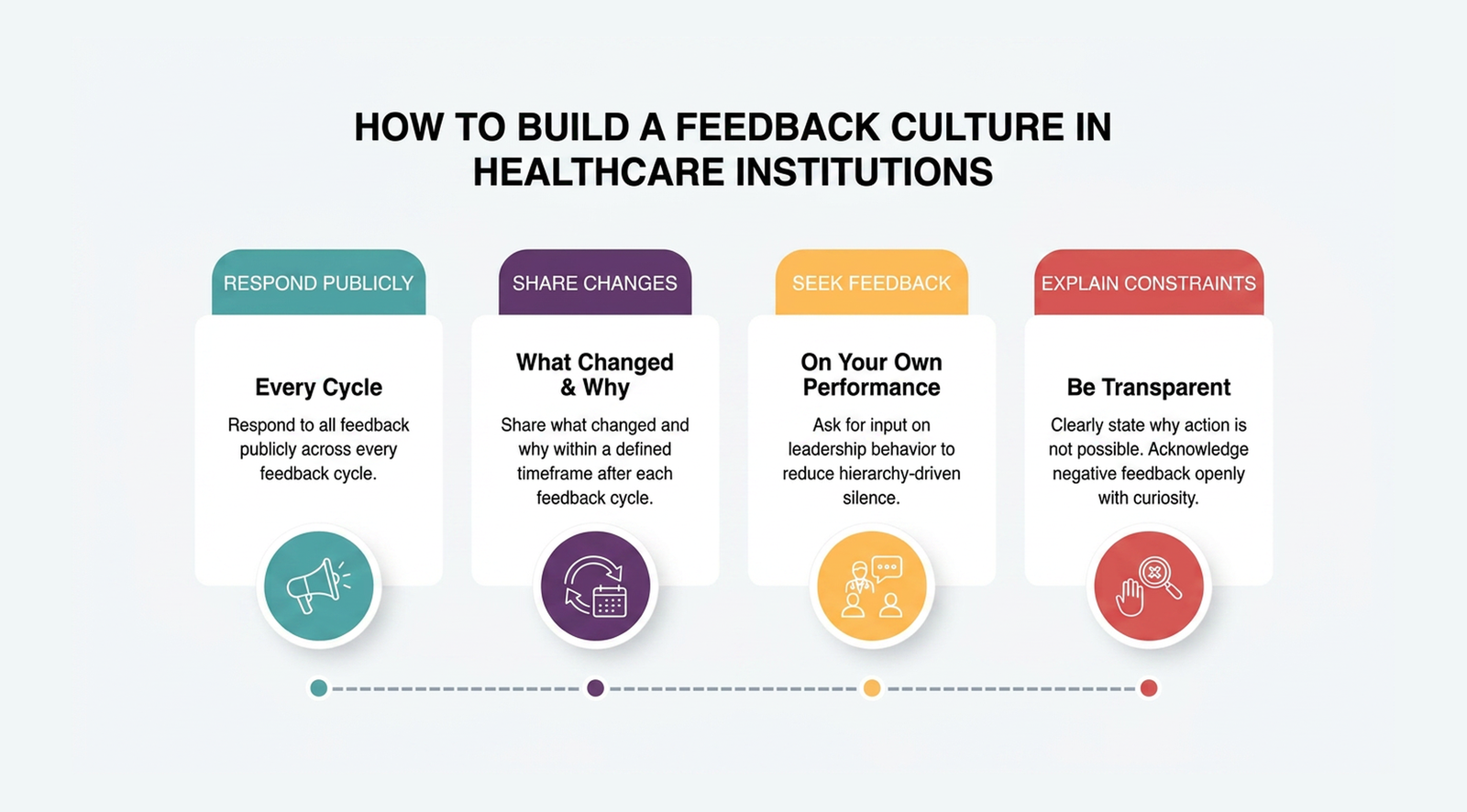
Clinical leaders build a feedback culture in healthcare by responding visibly to every feedback cycle, actively seeking input on their own performance, and explaining constraints when change is not possible.
The behaviors that build a feedback culture are specific and observable:
- Respond to every cycle publicly: Leaders must communicate what changed and why within a defined window after each feedback cycle. A response that arrives weeks later, or only to management, does not count as visible action.
- Seek feedback on your own performance: Leaders who ask for input on how they run meetings, communicate decisions, or handle escalations signal that hierarchy does not block honest exchange. This single behavior does more to reduce voice suppression than any policy.
- Explain constraints without deflecting: When feedback cannot lead to change, because of budget, policy, or capacity, leaders must say so directly and specifically. "We heard you, but cannot act on this right now because of X" preserves trust. Silence does not.
- Acknowledge negative feedback without defensiveness: Senior clinicians who receive critical input and respond with curiosity rather than justification model the behavior every junior staff member is watching for.
How do you train clinical managers to receive and act on feedback?

Training clinical managers to receive and act on feedback means shifting their role from recipients of information to facilitators of honest exchange. Most clinical managers are trained to give feedback on clinical performance, conduct, and competency, but not to receive it, sit with it, and respond to it without defensiveness.
Effective training for clinical managers covers four competencies:
- Receiving without reacting: Clinical managers must learn to hear feedback, including negative input about their own decisions, without immediately justifying, minimising, or redirecting. Training should include structured role-play where managers receive critical feedback and respond only with clarifying questions.
- Distinguishing facilitation from reception: Receiving feedback means listening. Facilitating feedback means actively creating the conditions under which staff feel safe to share honestly. Managers must understand both roles and know when each is required.
- Closing the loop at the unit level: Managers must be trained to translate feedback into named, visible actions within their own team and not to escalate all feedback upward and wait. Local loop closure is faster, more trusted, and more likely to sustain staff participation than organisation-wide reporting.
- Handling feedback that cannot be acted on: Clinical managers must learn to communicate constraints honestly and specifically. "This is outside my authority to change, and here is who I am escalating it to" is a complete response. "I will look into it" without follow-through is not.
Staff retention: Using staff insights to retain staff
What is a speaking-up culture in healthcare?
A speaking-up culture in healthcare is a specific condition in which clinical staff raise concerns, flag risks, and challenge decisions in real time, without waiting for formal channels, survey cycles, or scheduled reviews.
Speaking up fails in healthcare for the same structural reasons feedback fails, because of hierarchy, retaliation risk, and perceived futility, but the consequences of silence are immediate and clinical rather than organisational.
A functioning speaking-up culture in a healthcare institution shows three observable signs:
- Junior staff raise concerns during decision-making, not after. They do not wait for a debrief or an incident form. They speak in the moment, to the person with authority.
- Senior clinicians acknowledge and thank staff who speak up, publicly and consistently. This behavior signals that challenge is welcome, not punished.
- Teams debrief routinely after incidents and near misses, treating what was said and what was not said, as equally important data.
How do you launch a feedback program from scratch in a hospital?
Launching a feedback program from scratch in a hospital requires sequencing psychological safety before tools, anonymity controls before data collection, and visible action before any expectation of honest participation. Most hospital feedback programs fail because the sequence is wrong and surveys are deployed before staff believe speaking up is safe, and participation is low or dishonest as a result.
The correct launch sequence has five stages:
Stage 1: Establish psychological safety baseline
Before any feedback tool is deployed, clinical leaders must signal, through visible behavior, not policy statements, that honest input will be welcomed and acted on. This means senior clinicians publicly seek feedback on their own decisions, acknowledging prior failures to act on staff input, and committing to a defined response timeline. This stage takes weeks, not days.
Stage 2: Design anonymity controls for your team size
Identify which clinical units fall below the 10-person threshold where standard survey anonymity breaks down. For those units, configure aggregation thresholds, external facilitation routes, and delayed batch reporting before the first survey goes live. Anonymity must be structurally enforced, not merely promised.
Stage 3: Select channels matched to clinical workflows
Hospital staff operate across shifts, wards, and settings where desktop surveys are inaccessible. Launch with at least two channels, one pulse survey tool and one always-on channel such as a mobile-accessible form or QR code access point. Match the channel to where staff actually have a moment to respond: end of shift, during handover, or in break areas.
Stage 4: Run a single short cycle and close the loop visibly
The first feedback cycle should be short, five questions or fewer, and the response must be communicated within 14 days at the unit level. The first visible action is the most important of the entire programme. Staff are evaluating whether leadership will respond. One visible, named action from the first cycle does more to build lasting participation than any subsequent feature or incentive.
Stage 5: Establish a regular cadence and measure behavior, not completion rates
Set a consistent cycle, like monthly pulse surveys with quarterly deeper dives, and hold to it. Measure whether staff escalate concerns earlier, whether junior clinicians raise issues in team settings, and whether feedback leads to documented action within defined windows. Completion rate is a measure of tool adoption. Behavioral change is the measure of a functioning feedback culture.
(Source: CultureMonkey)
How to design anonymous feedback that works in small clinical teams?
Anonymous feedback in small clinical teams works by preventing identity inference through aggregation, external facilitation, team-size thresholds, and delayed reporting.
In small teams, healthcare workers often rely on informal signals, increasing the hospital anonymity challenge. These controls address the hospital anonymity challenge in low headcount units.
In an anonymous feedback clinical workforce, the core hospital anonymity challenge is that responses can be traced through context, timing, or writing style.
Why do feedback cultures collapse in healthcare institutions?
The feedback loop healthcare may collapse when staff see no visible response to what they shared. Without consistent, visible action, staff conclude that feedback is collected but not used, and participation drops. The absence of visible follow-through is the most common and preventable cause of feedback culture failure in clinical settings.
1. Make feedback closure communication routine
Translate feedback discussions into clear actions and communicate outcomes consistently. Staff should see what changed, why it changed, and how their input contributed. Leaders must actively participate in the feedback cycle, collecting, acting on, and communicating outcomes, to set the tone for the organization.
Use this report generator to input your team's feedback themes, the actions taken, timelines, and owners to get a clean, branded PDF you can share directly with your employees.
| Feedback received | Action taken | Timeline | Communicated by | Status |
|---|
If no action was taken, document the reason in the action column — transparency on constraints is as important as visible change.
2. Close the loop at the unit level
Share actions within the same clinical unit where healthcare feedback originated. Local visibility builds trust faster than organization-wide updates. Leaders should seek feedback on their own performance to normalize vulnerability and demonstrate the importance of feedback.
3. Acknowledge feedback even when no action is taken
Explain constraints when changes are not possible. Transparency maintains credibility and prevents perceived neglect. Leaders should openly discuss their mistakes and lessons learned to set a non-defensive tone in feedback conversations.
4. Show speed and consistency of response
Act on feedback within defined timelines and communicate progress. Delayed or inconsistent responses weaken trust in the system.
How to make feedback action visible in clinical settings
Making feedback action visible in clinical settings means communicating what changed, why it changed, and who acted on it, within the same unit where the feedback originated. Visibility is not a summary report sent to leadership. It is a direct, local response that staff can see and connect to what they shared.
The four practices that make action visible at unit level are:
- Translate feedback into named actions: Each feedback cycle should produce at least one specific change or a documented explanation of why change was not possible.
- Communicate within the originating team first: Share outcomes at unit level before organization-wide updates. Local visibility builds trust faster.
- Use a structured format every cycle: A consistent "you said, we did" format prevents responses from becoming ad hoc and easy to dismiss.
- Set and publish a response timeline: Define how many days separate feedback submission from visible response, and hold to it. Inconsistent timing is indistinguishable from inaction.

Conclusion
Building a feedback culture in healthcare institutions depends on creating conditions where staff feel safe to speak, trust the process, and see action. Hierarchy, anonymity gaps, and inaction are the main failure points. Addressing these requires structured systems, clear accountability, and consistent response behavior across clinical settings.
To operationalize this at scale, evaluate the leading healthcare workforce engagement tools built for continuous listening and action tracking.
CultureMonkey enables secure, multi-channel feedback collection, anonymity controls for small teams, and real-time dashboards that drive visible action. It helps healthcare institutions operationalize feedback, close loops, and build lasting trust across clinical teams. A strong culture of feedback directly improves patient care, team alignment, and organizational quality.
Book a demo with CultureMonkey.
Last reviewed: April 2026. This content reflects current clinical feedback research as of the publication date.
FAQs
1. How do you build a feedback culture in a hospital?
Build psychological safety before deploying tools. Staff must believe speaking up is safe. Enforce genuine anonymity, demonstrate visible action on prior feedback, and train clinical managers to facilitate input rather than just receive it. Tools without these foundations produce only compliance-driven responses.
2. What is psychological safety in a healthcare context?
Psychological safety in healthcare means staff can raise clinical concerns, give honest feedback, or challenge decisions without risking career consequences, team exclusion, or punitive response. It is the foundational condition for honest feedback and voluntary incident reporting in clinical settings.
3. Why do clinical staff fear giving feedback?
Four structural barriers suppress clinical feedback: hierarchy intimidation from senior clinicians, retaliation risk tied to career impact, perceived futility when prior input goes unaddressed, and anonymity doubt in small teams where responses feel identifiable despite anonymous survey systems.
4. How do you make feedback anonymous in a small clinical team?
Standard anonymity fails in teams under 10 since response patterns are identifiable. Use these controls: aggregate responses only at a 5-plus threshold, route collection through external facilitation, combine adjacent team data, and offer voluntary open-attribution for staff who prefer it.
5. What is the role of leadership in building a healthcare feedback culture?
Leaders build a feedback culture by responding visibly to every feedback cycle, actively seeking input on their own performance, and explaining why change is not always possible. Absent or inconsistent leader response is the most common cause of feedback culture failure in healthcare institutions.
6. How do you measure whether a feedback culture is working in a healthcare institution?
Measure behavioral signals, not just participation rates. A functioning culture shows in whether staff proactively escalate concerns, whether junior clinicians challenge decisions without consequences, and whether feedback consistently leads to documented visible action within defined response windows.
7. How does a feedback culture affect patient safety outcomes in hospitals?
Feedback culture directly affects patient safety. Clinical environments where staff feel safe to speak up report earlier escalation of patient risks, lower near-miss concealment rates, and stronger voluntary incident reporting. Hierarchy-driven silence raises patient safety exposure across clinical teams.






{kind=link}