

Employee engagement strategy for healthcare systems: 2026 guide
An employee engagement strategy for healthcare systems is a structured, multi-layered approach that aligns clinical, non-clinical, and administrative staff with patient outcomes, operational continuity, and regulatory demands.
Unlike standard models, it must function across a 24/7 workforce, credentialed roles, and multi-site complexity.
This guide covers clinical, non-clinical, and administrative engagement, measurement by site and shift, survey participation, calendar planning, and multi-site governance.


- An employee engagement strategy for healthcare systems is a role-based approach aligning clinical, operational, and admin staff with care outcomes and system performance.
- Generic engagement models fail because they ignore hierarchy, shift work, and patient-impact pressures in hospitals.
- The Workforce Archetype Model splits engagement into three tracks: clinical, non-clinical, and administrative.
- Engagement works when aligned to drivers, timed to system cycles, and adapted across sites.
- CultureMonkey enables this with multilingual, frontline-ready surveys and real-time dashboards for role-based, multi-site healthcare engagement.
Last reviewed: April 28, 2026. Reviewed for relevance to healthcare workforce engagement strategy and employee feedback practices.
What makes employee engagement in healthcare different?
Healthcare engagement strategies are different because they must work within a regulated workforce, a 24/7 operating model, and direct accountability to patient outcomes. These conditions define a healthcare employee engagement strategy and what makes it different from standard models used in other industries.
Healthcare employee engagement differs from corporate engagement because hospitals operate with licensed roles, shift-based staffing, and direct patient-safety accountability.
Three structural factors define this:
- Regulated workforce: Clinical roles follow strict licensing, protocols, and hierarchy. Healthcare engagement barriers appear when engagement ignores these limits on autonomy and decision-making.
- 24/7 operating model: Hospitals never stop, making 24/7 workforce engagement essential. Shift work and rotation patterns break standard communication and feedback systems.
- Patient-outcome accountability: Engagement directly affects care quality and safety. Disengagement is not cultural, it impacts real clinical decisions and outcomes.
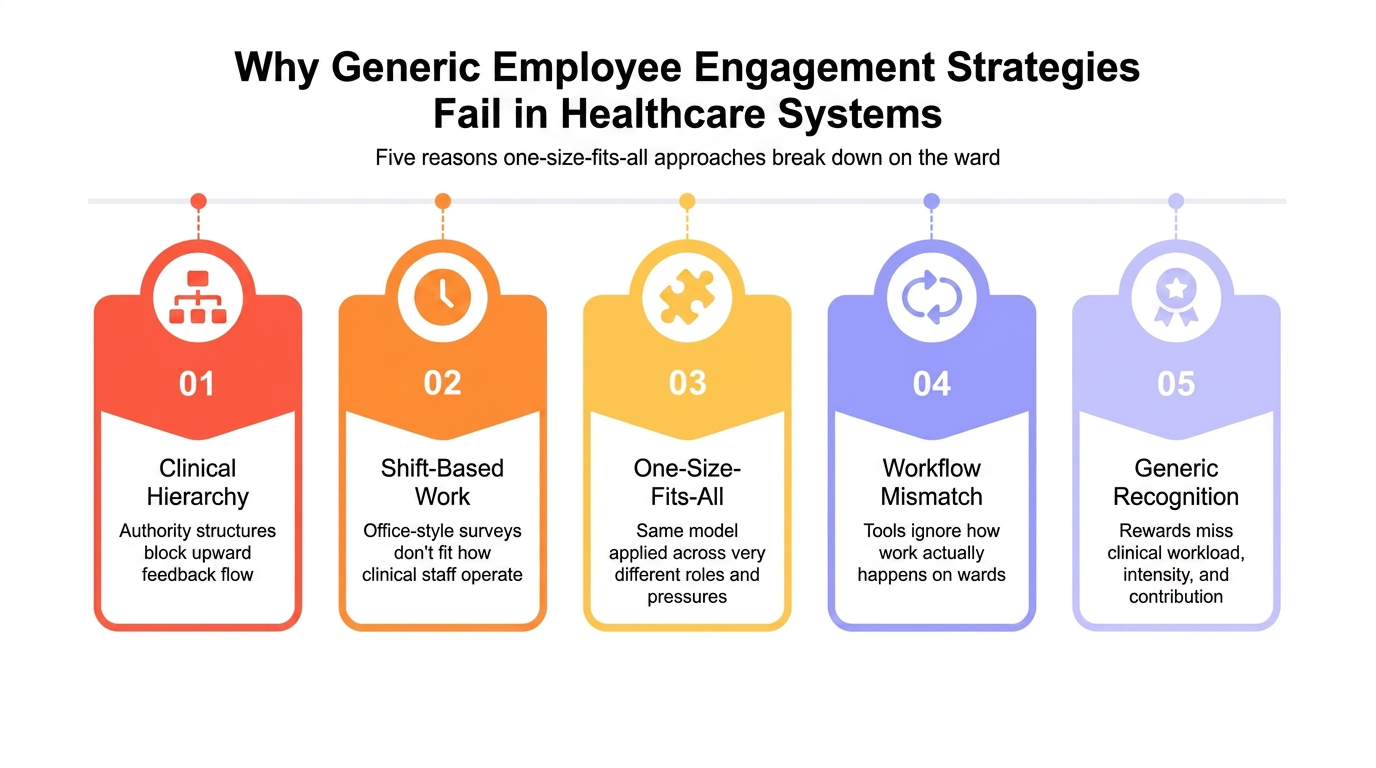
Why generic engagement models fail in hospitals

Generic engagement frameworks fail in healthcare for three reasons: they ignore clinical hierarchy, assume office-based work, and apply the same engagement model to very different roles.
An overview of employee engagement strategies built for corporate settings does not fit hospital environments, which is why hospital staff are disengaged. This is why engagement strategies fail healthcare because generic frameworks built outside clinical environments cannot translate into hospital settings.
Ignoring credentialing hierarchy
- Clinical work follows strict authority structures, not open feedback systems.
- Hospital employee engagement problems increase when engagement assumes everyone can speak equally.
- Feedback often breaks because hierarchy limits how issues move upward.
Applying office-designed surveys to ward environments
- Most engagement tools assume desk access and predictable schedules.
- Employee engagement challenges in hospitals increase when staff cannot respond during shifts.
- Surveys miss real sentiment because they do not fit how work happens on the floor.
One-size-fits-all recognition models
- Recognition programs ignore differences in workload, pressure, and responsibility.
- Hospital HR challenges 2025 include building engagement that reflects real job intensity.
- Generic rewards fail because they do not match clinical contribution or constraints.
The Workforce Archetype Model for healthcare systems
The Workforce Archetype Model explains healthcare engagement as three distinct systems, not one unified program. Clinical vs non-clinical staff engagement cannot be managed through the same methods because roles, constraints, and motivations differ structurally.
The Workforce Archetype Model divides healthcare engagement into clinical, non-clinical operational, and administrative tracks so each workforce segment is managed using role-relevant drivers and real operating constraints.
Three tracks define the system:
Track 1: Clinical (credentialed workforce)
- Operates under licensing, protocols, and strict hospital hierarchies engagement.
- Frontline healthcare worker disengagement is driven by pressure, limited autonomy, and constrained feedback loops.
- Clinical employee silence is often structural, not cultural, due to escalation barriers and authority layers.
Track 2: Non-clinical operational (support workforce)
- Includes facilities, housekeeping, food services, and transport roles.
- Engagement depends on shift equity, visibility, and access to communication.
- Employee engagement use cases in healthcare often fail here due to lack of inclusion in hospital workforce engagement plan design.
Track 3: Administrative (system coordination layer)
- Includes HR, finance, compliance, and planning functions.
- Responsible for aligning policy, communication, and execution across tracks.
- Engagement depends on connecting role output to patient and system outcomes.
How to build a healthcare engagement strategy in five steps?
Effective healthcare engagement works when each workforce segment is managed on its own term, with the right survey channel, the right cadence, and a named action owner. The table below maps each track to its core driver, measurement approach, and success signal.
| Step | Action | Owner |
|---|---|---|
| 1 | Segment workforce into clinical, non-clinical, and administrative tracks | HR lead |
| 2 | Map engagement drivers per track using the Workforce Archetype Model | HR + ops |
| 3 | Design survey channels and cadence to fit each track's access constraints | HR + IT |
| 4 | Align engagement calendar to system pressure cycles | HR + site leads |
| 5 | Set action owners and review loops at both central and site level | Senior leadership |
How to improve engagement for clinical staff?
Clinical staff engagement improves when hospitals protect autonomy, support skill development, and align operations with patient-care values. Clinicians disengage when hierarchy blocks feedback or policies conflict with safe care. Effective clinical engagement must fit licensed practice, shift intensity, and escalation constraints.
Autonomy
- Control over decisions within clinical scope.
- Engagement drops when judgment is restricted.
Mastery
- Continuous skill development and progression.
- Static roles reduce commitment.
Moral alignment
- Work must align with patient care values.
- Mismatch between operations and care breaks engagement.
(Source: Gallup)
How to improve engagement for non-clinical hospital teams?
Non-clinical staff engagement improves when support roles are visible, shifts are distributed fairly, and operational teams are included in recognition. Housekeeping, transport, and facilities staff disengage when engagement programs skip them entirely. Effective engagement must match their shift access and communication constraints.
Recognition visibility
- Work is often unseen but essential to daily operations.
- Engagement improves when contributions are visible and acknowledged.
Shift equity
- Work is spread across shifts, often with uneven conditions.
- Engagement drops when schedules feel unfair or inconsistent.
Role dignity
- Roles are operational but critical to how the system runs.
- Engagement depends on respect, inclusion, and access to communication.

Take time to appreciate employees and they will reciprocate in a thousand ways.
Dr. Bob Nelson

![]()
Author, Keynote Speaker & Employee Engagement Consultant
How to improve engagement for administrative teams in health systems
Administrative staff engagement improves when roles are clearly linked to patient outcomes, not just internal processes. The distance from direct care creates a purpose gap that generic programs miss. Connecting admin decisions to frontline impact is the core engagement driver for this group.
Outcome and purpose
- Work is removed from direct patient care.
- Engagement improves when roles clearly link to care outcomes.
Operational visibility
- Administrative decisions shape how care is delivered.
- Engagement improves when teams see how their work affects the frontline.
System alignment
- Roles sit across functions, policies, and processes.
- Engagement depends on clear links between clinical needs and admin decisions.
How do you improve survey participation in hospital teams?
Survey participation drops when tools require desktop access, surveys are too long, or staff distrust anonymity. Use mobile-first, multilingual pulses under five questions during peak periods, and visibly close the feedback loop so staff see changes linked to their input.
Why participation drops
- Desktop-only tools exclude shift-based staff who have no screen access during work
- Surveys longer than five questions lose frontline staff during high-pressure periods
- Staff disengage permanently when feedback disappears with no visible action taken
How to improve it
- Use mobile-first, multilingual tools accessible during or between shifts
- Keep pulses under five questions during peak-pressure windows
- Close the feedback loop visibly so staff see changes linked to their input
Why frontline and admin need separate channels
- Access patterns differ: Frontline staff cannot use desktop surveys mid-shift
- Language needs vary: Non-clinical staff often need multilingual survey options
- Trust baselines differ: Frontline staff need stronger anonymity assurances than admin teams
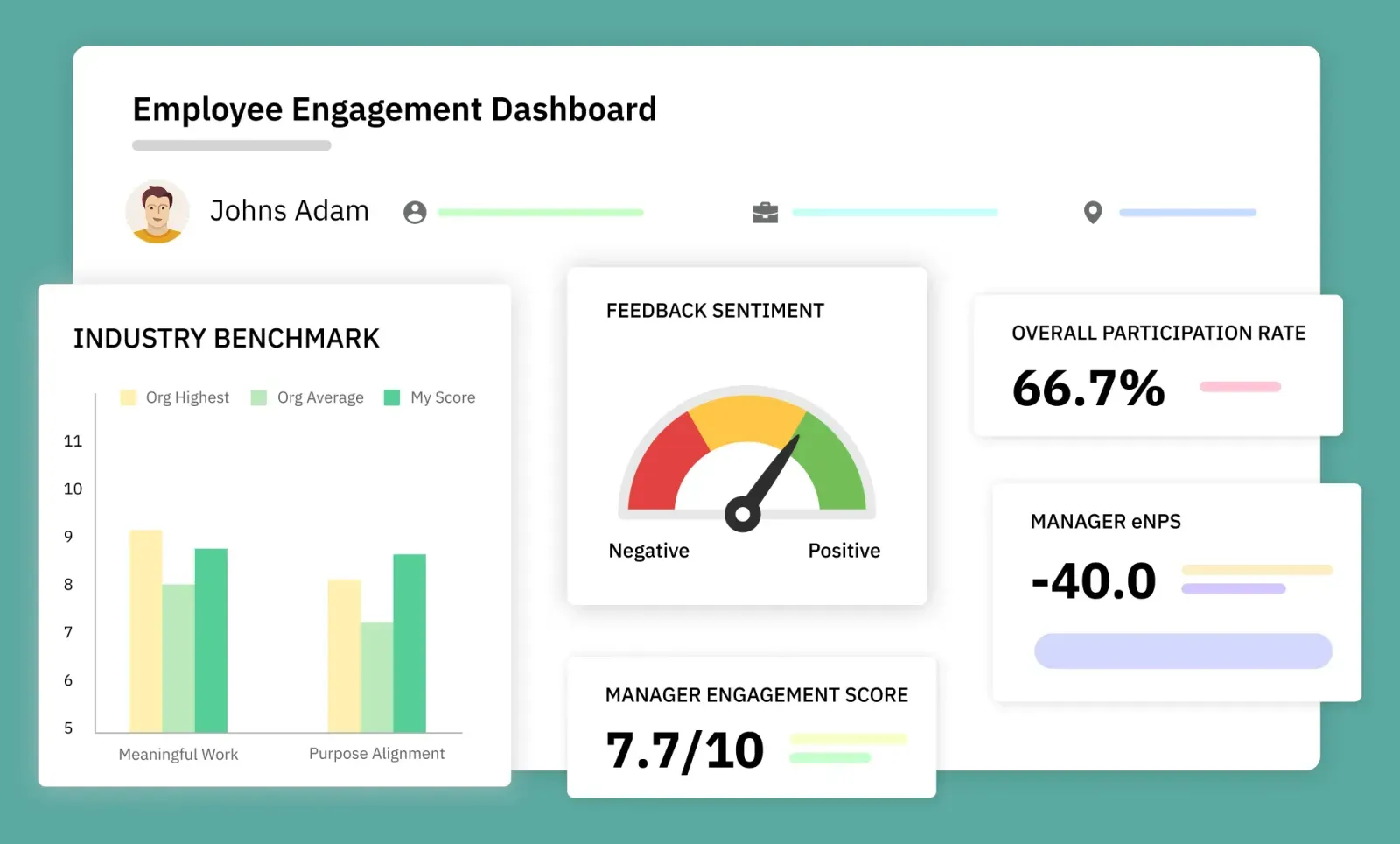
How healthcare systems should measure employee engagement
Healthcare systems should measure engagement by segmenting results across workforce type, site, and shift, not a single systemwide score. Pulse surveys, anonymous feedback, and action-tracking dashboards work best when reviewed separately at ward, department, and system level.
| Track | Top driver | Survey channel | Review cadence | Action owner | Success metric |
|---|---|---|---|---|---|
| Clinical | Autonomy + moral alignment | Mobile pulse, anonymous | Monthly | Ward lead + HR | Reduction in clinical silence signals |
| Non-clinical | Recognition + shift equity | SMS or paper backup | Bi-monthly | Facilities manager | Participation rate by shift |
| Administrative | Purpose connection | Desktop survey | Quarterly | Dept head + HR | Engagement score linked to care outcomes |
How to build a health system engagement calendar?
Building a health system engagement calendar requires a healthcare workforce engagement plan aligned to how pressure shifts across the year. The engagement timeline must reflect accreditation cycles, winter pressure, and contract transitions.
Using engagement strategies in hospitals works only when timing matches real operating conditions.
Rule 1: Adjust engagement during peak pressure
- During winter pressure, keep engagement short and low effort.
- Top employee engagement strategies in healthcare here are quick and actionable.
Rule 2: Match engagement to system cycles
- Accreditation periods → clarity, compliance, readiness
- Contract or role transitions → communication and stability
- Stable periods → deeper engagement and analysis
Rule 3: Design for timing, not repetition
- Engagement effectiveness depends on when it runs, not how often.
How to govern engagement across a multi-site health system?

Governing engagement across a multi-site health system requires a clear operating model for ownership, consistency, and local adaptation. Large health system engagement governance is not about central control alone. It defines how engagement across hospitals is structured, measured, and acted on without losing site-level relevance.
Central standards
- Define what is measured, how often, and at what level.
- Ensure consistency in engagement design across all hospitals.
Local ownership
- Site leaders act on engagement insights within their context.
- Engagement actions must reflect local workforce and operational conditions.
Data alignment
- Use a shared framework to compare engagement across hospitals.
- Maintain visibility without forcing uniform responses.
Decision loops
- Set clear pathways from feedback to action at both central and site levels.
- Avoid delays caused by unclear ownership.
Healthcare workforce engagement framework is defined centrally, but engagement is driven locally based on context. If you want to know how to improve employee engagement in healthcare, read more on employee experience strategy for hospital networks.
How does engagement strategy differ across hospital types?
Common mistakes in healthcare engagement strategy
Healthcare engagement strategies fail when they treat the entire workforce as one group. The most common mistakes, wrong timing, missing feedback loops, and excluded staff groups, are structural, not cultural. Each one is preventable with role-based design.
Using one engagement approach across all hospital roles
- Applying the same surveys and actions to clinical, operational, and administrative staff ignores how work differs
- Results in low participation, poor insights, and weak action plans
- Fix: segment engagement by workforce type before designing any program
Surveying without closing the feedback loop
- Staff stop responding when they see no changes linked to their input
- Trust in the engagement process breaks fastest on frontline and non-clinical teams
- Fix: assign a named action owner to every survey cycle
Timing engagement against the wrong cycles
- Running deep diagnostics during winter pressure or accreditation periods kills participation
- Fix: align survey cadence to system pressure points, not calendar quarters
Ignoring non-clinical staff in engagement design
- Facilities, housekeeping, and transport teams are routinely excluded from program design
- Fix: include non-clinical access constraints and language needs from the start

Conclusion
An employee engagement strategy for healthcare systems works when it reflects how hospitals actually operate. Segmenting the workforce, aligning engagement to clinical realities, and timing initiatives to system pressure are what make strategies effective. Generic models fail because they ignore these conditions, while structured approaches drive measurable outcomes.
CultureMonkey enables this by supporting role-based engagement design, multi-site governance, and real-time insights. With multilingual surveys, frontline-friendly access, and actionable dashboards, it helps health systems implement and scale engagement strategies effectively.
Book a demo with CultureMonkey.
FAQs
1. What is an employee engagement strategy for healthcare systems?
An employee engagement strategy for healthcare systems is a role-based plan that improves commitment, communication, and retention across clinical, operational, and administrative teams. It must fit shift work, regulation, patient-care pressure, and multi-site coordination to be effective.
2. Why do generic engagement frameworks fail in hospitals?
Generic engagement frameworks fail in hospitals because they assume desk-based work, open communication, and uniform motivation. Healthcare teams operate within hierarchy, rotating shifts, credentialing rules, and patient-care pressure, so generic surveys and actions miss real barriers daily.
3. How should hospitals measure employee engagement?
Hospitals should measure employee engagement by segmenting results by workforce type, site, function, and shift rather than using one systemwide average. Pulse surveys, anonymous feedback, manager follow-up, and action tracking work best when tied to operational and care-delivery realities.
4. What are the main drivers of clinical staff engagement?
The main drivers of clinical staff engagement are autonomy, mastery, and moral alignment. Clinicians stay engaged when they can use judgment within scope, keep developing skills, and see that operational decisions support safe patient care instead of undermining professional values at work.
5. How can a multi-site health system govern engagement consistently?
A multi-site health system governs engagement consistently by setting central standards for measurement, survey cadence, and reporting while allowing local leaders to act on context-specific issues. This model protects comparability across hospitals without forcing identical actions everywhere.
6. What should a healthcare engagement calendar include?
A healthcare engagement calendar should reflect operational pressure points such as accreditation reviews, winter demand, staffing transitions, and recovery periods. Short pulses fit peak-pressure windows, while deeper diagnostics and action planning should happen during more stable operating periods.
7. What is the difference between employee engagement and employee experience in healthcare?
Employee engagement measures how committed and motivated staff are in their roles. Employee experience covers everything that shapes that commitment, such as the environment, tools, processes, and culture. In healthcare, engagement is the outcome; employee experience is the system that drives it.







{kind=link}