

Measuring engagement across hospital departments in 2026
Measuring employee engagement across hospital departments requires a department-specific approach that accounts for differences in workload, schedule patterns, acuity, and role context. Uniform surveys applied across ICU, ED, wards, and admin teams produce misleading scores that lead to ineffective interventions and missed retention risks.
An ICU team operating under sustained high acuity, rotating 12-hour shifts, and chronic moral distress will score differently from an administrative team with predictable hours and low emotional labor, not because one is more engaged, but because the instruments weren't designed for their context.
This guide builds a department-level measurement architecture that accounts for clinical reality.


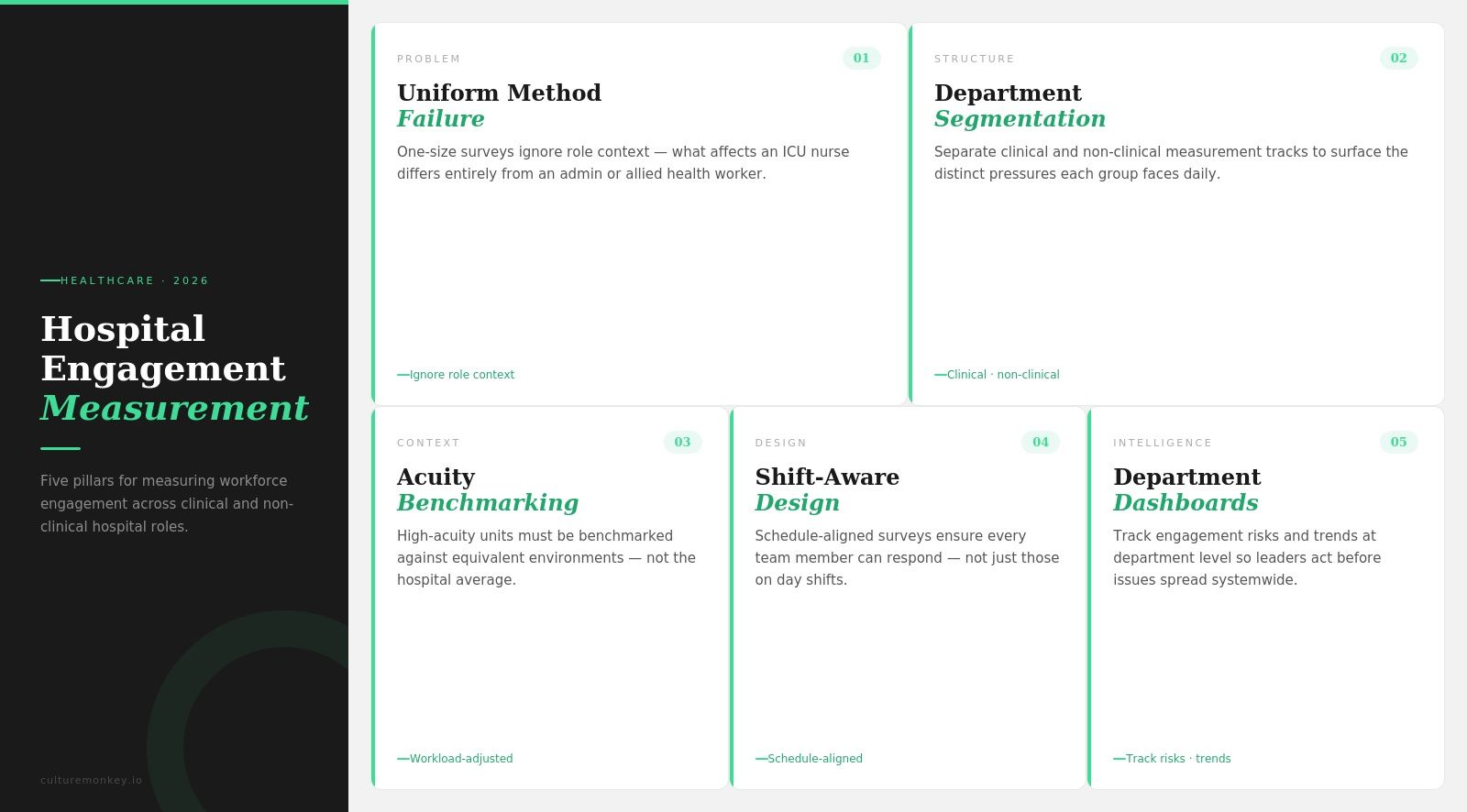
Measuring engagement across hospital departments means evaluating each unit by workload, shifts, and clinical context.
- Uniform surveys distort data because ICU, ED, ward, and admin teams operate under different pressures.
- Department segmentation separates clinical, non-clinical, and support teams by operating reality, not org chart position.
- Acuity-adjusted benchmarking prevents misleading comparisons by evaluating engagement scores against units with similar workload intensity.
- Shift-aware survey design improves participation by matching format, timing, and channel to actual clinical workflows.
- Department-level dashboards help leadership identify engagement gaps, root causes, and trends at the unit level.
- CultureMonkey enables measuring engagement across hospital departments using multi-channel surveys, benchmarking, anonymity controls, and dashboards.
Why does measuring engagement the same way across all hospital departments fail?

Measuring engagement across hospital departments fails when hospital employee engagement is measured using the same surveys, benchmarks, and assumptions across clinical and non-clinical units, ignoring differences in workload, risk, schedules, and role context, leading to misleading insights and weaker decisions.
1. Acuity distorts the baseline
ICU teams work in constant urgency, emotional load, and higher clinical risk, while admin teams operate in steadier environments. When healthcare organizations score both with the same benchmark, measuring engagement across hospital departments turns context into noise and makes employee engagement look weaker or stronger than it really is.
2. Workflow access skews participation
Standard surveys often assume desk access, email visibility, and predictable work hours. Many healthcare workers do not have that reality. If response design ignores shifts, handoffs, and floor-based work, healthcare employee engagement data gets shaped by who could answer, not by who actually felt engaged across hospital departments.
3. Role context changes what engagement means
A nurse, a lab technician, and a billing coordinator do not experience support, autonomy, or pressure in the same way. Using a single fixed question set across departments makes hospital employee engagement measurement too generic, hiding the real drivers of employee engagement across different healthcare organizations.
4. Leadership decisions are built on false comparisons
Once non-comparable scores sit on the same dashboard, leaders start treating unlike departments as if they have the same problems. That pushes the wrong action plans, weakens trust in measuring engagement across hospital departments, and makes healthcare workers feel surveyed without being properly understood.
5. Standard surveys flatten department-specific signals
What looks like low engagement in one unit may actually reflect understaffing, patient intensity, or schedule strain rather than culture alone. Without structural adjustment, healthcare employee engagement insights lose precision, and healthcare organizations miss the operational causes sitting underneath the score when measuring engagement across hospital departments.
6. Trend lines become misleading over time
If one department has stable routines and another faces rotating shifts, floating staff, and emergency surges, year-on-year comparisons break down fast. Good hospital employee engagement measurement tracks employee engagement within the right departmental frame before comparing anything across healthcare organizations when measuring engagement across hospital departments.
What is the department segmentation model for hospital engagement measurement?
A department model for hospital engagement measurement must reflect real differences in workload, pace, and pressure across ICU, ED, wards, allied health, and admin.
When these units are grouped too broadly, the data becomes inaccurate, limiting decision-making and reducing the effectiveness of engagement actions.
- Segment by operating reality: Start with hospital unit measurement that separates ICU, ED, wards, allied health, and admin by work pattern, not org chart alone. This makes a department-level hospital engagement survey design more usable, because employee experience differs sharply across pace, risk, and coordination load.
- Match cadence to unit pressure: High-intensity units need shorter, more frequent check-ins, while lower-volatility teams can sustain a slower rhythm. That is central to how to measure nurse engagement well, because healthcare staff in fast-moving settings cannot respond reliably to long surveys sent at fixed intervals.
- Use format by access point: Choose QR, kiosk, text messages, mobile, or supervised formats based on where healthcare providers actually work. When employees engaged on the floor have limited email access, the right response channel helps improve employee well-being by making participation easier across the healthcare system.
- Benchmark within department groups: Benchmarking within peer department groups prevents patient care decisions from being driven by misinterpreted engagement scores, because a low ICU score may reflect sustained workload strain, while the same score in admin signals a fundamentally different problem.
- Separate core and unit-specific questions: Keep a small shared question set for comparison, then add unit-level questions tied to workload, support, and team flow. This lets employee engagement matters stay visible at the system level, while mental health and local barriers are measured where they actually happen.
- Report action at the manager level: Dashboards should show results by department, shift pattern, and role cluster so leaders can act precisely. A strong department-level engagement survey hospital model helps healthcare staff see that feedback changes work conditions, which builds trust and keeps employees engaged over time.
What is acuity-adjusted benchmarking, and why should ICU scores never compare to admin scores?
Measuring engagement across hospital departments requires adjusting for clinical acuity before comparing scores. ICU, ED, and admin teams operate under different workloads, risks, and pressures. Without acuity-adjusted benchmarking in healthcare, employee surveys produce misleading results and weaken hospital engagement benchmarks by department.
How do you design shift-aware engagement surveys for clinical staff?
Shift-aware survey design for clinical staff requires aligning survey timing with real shift schedules, workload patterns, and availability across the healthcare workforce. If shift-based engagement survey healthcare design ignores these factors, response rates drop, and feedback fails to reflect actual job satisfaction and working conditions accurately.
- Use QR kiosks in break zones: Place quick-response kiosks in staff rooms, cafeterias, and nurse stations to capture feedback during natural pauses. This supports nurse engagement survey design by reducing dependence on email and administrative tasks for healthcare professionals working continuous clinical shifts.
- Trigger surveys between shifts: Send short WhatsApp or mobile pulses during shift transitions, when the healthcare workforce's attention is briefly available. This improves response rates and helps healthcare leaders collect valuable insights without interrupting care delivery or impacting clinical outcomes across the health system.
- Embed feedback into clinical handovers: Introducing one or two targeted engagement questions during shift handover moments makes feedback collection a routine clinical activity rather than an extra task. This approach captures real-time workload, coordination, and job satisfaction data from clinical staff without requiring additional surveys or separate sessions
- Protect anonymity in small teams: In tightly knit units, responses can feel identifiable. Use thresholds and grouped reporting to ensure privacy, so healthcare professionals feel safe sharing honest input, which helps enhance engagement and builds trust with senior management across healthcare facilities.
- Design ultra-short survey formats: Keep surveys under 60 seconds with focused questions tied to immediate experience. This respects time pressure in the healthcare industry while still providing valuable insights that reflect real conditions without overwhelming the healthcare workforce.
- Align survey timing with care intensity: Avoid sending surveys during peak clinical hours or emergency-heavy periods. Timing surveys correctly helps healthcare leaders capture cleaner data, ensuring feedback reflects actual job satisfaction rather than temporary stress spikes in high-pressure environments.
How do you run engagement surveys when staff don't have email access?
Running surveys for clinical staff without email requires methods aligned with real workflows, limited access, and time constraints. Measuring engagement among frontline healthcare workers must include mobile, kiosk, or assisted formats. When clinical staff without email are excluded, response rates drop, and insights fail to reflect patient needs and care quality.
- Use mobile-first survey access: Test messages links and QR codes allow clinical staff without email to respond quickly during shifts. This supports a continuous process, improves response rates, and captures satisfaction levels tied to real care delivery without disrupting workflows or patient needs.
- Place kiosks in high-traffic areas: Break rooms, nurse stations, and locker zones allow quick participation without needing personal devices. This improves response rates, supports open communication, and helps capture key drivers behind patient experience and care quality across units.
- Introduce verbal-assisted survey prompts: Supervisors can guide new employees and travel nurses through survey intent without influencing answers. This improves participation, surfaces safety issues early, and supports better decision-making by capturing feedback from those often missed in standard processes.
- Use anonymised paper fallback methods: In restricted or low-connectivity units, paper surveys ensure no group is excluded. Paper-based collection protects data coverage, helps track absenteeism and retention trends, and ensures clinical and support staff in low-connectivity environments are not systematically excluded from engagement measurement.
- Keep surveys short and frequent: Short formats improve completion in time-constrained environments and support a continuous process. This helps track net promoter score trends, well-being signals, and satisfaction levels without overloading clinical teams.
- Group and report data carefully: Small teams require threshold-based reporting to maintain trust. This improves open communication, increases response rates over time, and ensures insights reflect true engagement rather than fear of identification.
How do you build a hospital engagement dashboard by department?
A hospital engagement dashboard organises department-level survey results into clear, actionable insights. HR analytics healthcare uses this structure to identify specific areas, track engagement levels, and improve operational efficiency across units by linking data to decisions, trends, and measurable outcomes.
- Show hospital engagement score by unit: Display each department separately to reflect true engagement levels across the organisation. This helps identify areas where employee engagement in healthcare differs, aligns with industry standards, and improves the overall work environment through targeted strategies.
- Add trend lines for each department: Track survey results over time within units to reveal patterns and root causes. This helps leaders identify specific areas needing attention and tailor interventions that improve employee satisfaction and sustain highly engaged teams.
- Overlay acuity and workload context: Combine engagement data with workload and care intensity to avoid misinterpretation. This ensures insights reflect the real work environment and helps healthcare teams focus on factors that influence both employee satisfaction and patient satisfaction.
(Source: SHRM)
- Break down by shift and role segments: Segment data by shifts and job roles to capture differences across teams. This helps identify areas where engagement levels vary, supports targeted strategies, and improves operational efficiency without relying only on existing systems.
- Map key drivers to outcomes: Link engagement data to drivers like leadership, workload, and recognition. This provides actionable insights, helps organizations invest in the right talent, and supports better decision-making across the work environment.
- Enable action through manager dashboards: Provide department-level access so leaders can act on feedback quickly. This helps tailor interventions, address root causes, and ensure survey results lead to visible improvements in engagement levels and team performance.
How should you present department-level engagement data to clinical leadership?
Presenting department-level engagement data to clinical leadership works best when findings are translated into the metrics leaders already track: safety incidents, staffing stability, and accreditation readiness. Engagement reports framed in operational language drive action; those framed as standalone HR metrics do not.
- Translate engagement into patient safety metrics: Map low engagement areas to incident rates, escalation delays, and reporting gaps. This helps leaders see how engagement affects safety outcomes and supports stronger accountability in clinical environments.
Example: If ICU engagement drops 12% while staffing strain increases, link it to outcomes. Safe staffing is associated with 14% lower mortality, 20% better infection prevention, and shorter ICU stays. Recommend reviewing staffing ratios and shift coverage immediately. (Source: NIH)
- Connect data to staffing stability: Show how engagement links to absenteeism, overtime dependency, and retention trends. This helps leadership understand workforce pressure and act before gaps affect care delivery.
Example: If engagement declines alongside rising absenteeism and overtime in a ward, flag staffing risk and recommend workload redistribution or hiring adjustments. - Align with accreditation and compliance measures: Present engagement alongside audit readiness, documentation quality, and compliance scores. This positions engagement as a driver of regulatory performance, not just a people metric.
- Focus on unit-level clarity, not averages: Break data by department instead of presenting hospital-wide scores. This helps leaders identify where problems exist and avoid decisions based on diluted averages.
- Highlight drivers, not just scores: Show what is causing engagement changes, such as workload, leadership support, or communication gaps. This gives leaders a clear path to action rather than leaving them with surface-level data.
- Show trends and movement over time: Present how engagement is improving or declining across reporting periods. This helps leadership evaluate whether interventions are working and where further attention is needed.
- Tie insights to clear actions: End every report with recommended next steps linked to specific issues. This ensures engagement reporting hospital leadership drives decisions, not just discussion.
What are hospital engagement survey questions for clinical vs non-clinical departments?

Hospital engagement survey questions must differ by department because clinical and non-clinical teams experience work differently. Clinical roles focus on patient care, urgency, and safety, while non-clinical roles manage processes and coordination. Using the same questions leads to incomplete insights and weak decisions.
What do healthcare employee engagement benchmarks look like by department?
Healthcare employee engagement benchmarks by department must reflect differences in workload, acuity, and shift patterns across units. A single hospital-wide benchmark creates misleading comparisons. Effective benchmarks define what stable, improving, and at-risk engagement looks like within each department’s real working conditions.
- Benchmark within comparable units: ICU, ED, wards, allied health, and admin should each have separate benchmark ranges. This makes comparison fairer, helps leaders read scores in context, and prevents department-level engagement data from being distorted by workload intensity, patient risk, and role demands.
- Use trend ranges, not fixed targets: A useful benchmark shows whether a department is stable, improving, or declining over time. This approach helps hospitals avoid chasing static numbers and instead focus on movement, consistency, and whether local engagement conditions are getting stronger or weaker.
- Adjust for acuity and shift load: High-acuity units and rotating-shift teams need benchmark ranges that reflect sustained pressure. Without that adjustment, lower scores may be misread as a weak culture, when the real issue is workload strain, fatigue, or the demands of continuous patient care.
- Separate role-based patterns inside departments: Nurse, technician, and support-role benchmarks may differ even within the same unit. This helps hospitals identify where engagement pressure sits most sharply, instead of assuming one department score reflects the full experience of every role inside it.
- Pair benchmark scores with response context: Participation rates, survey channel, and shift coverage should sit beside benchmark data. This makes the benchmark more trustworthy, because leaders can see whether the score reflects broad department input or only the staff who had the easiest access.
- Link benchmark bands to action thresholds: Good benchmarks should trigger different responses for stable, warning, and high-risk ranges. This turns engagement measurement into an operating tool, helping managers decide when to monitor, when to investigate, and when immediate department-level intervention is needed.
Conclusion
Measuring engagement across hospital departments is essential because each unit operates under different pressure, workload, and risk. Without it, decisions rely on incomplete data, leading to ineffective interventions and missed risks in patient care and staffing.
CultureMonkey enables healthcare organizations to measure engagement with precision through department-level segmentation, shift-aware surveys, and real-time dashboards.
CultureMonkey's multi-channel distribution ensures frontline inclusion, even without email access. With actionable insights, anonymity controls, and manager-level reporting, CultureMonkey helps leaders identify gaps early, tailor interventions, and build a more responsive, high-performing healthcare environment grounded in accurate engagement measurement.
FAQs
1. How do you measure employee engagement in a hospital?
Measure hospital employee engagement using a multi-channel approach segmented by department. Use QR kiosks and mobile surveys for clinical staff, WhatsApp pulses for shift teams, and digital forms for admin. Benchmark within department groups, not across them, to avoid misleading comparisons between units.
2. What is acuity-adjusted engagement benchmarking in healthcare?
Acuity-adjusted benchmarking controls for clinical patient load when comparing engagement scores across hospital units. High-acuity departments like the ICU and ED face structural pressure that lowers scores artificially. Comparing them only against equivalent units prevents misdirected leadership decisions.
3. Should hospital departments have different engagement benchmarks?
Yes. Clinical units with high patient acuity, emotional labor, and critical care exposure must be benchmarked only against similar departments. A single hospital-wide benchmark demoralizes high-performing clinical teams with low scores and masks genuine disengagement in lower-pressure support functions.
4. Can you run effective surveys with shift-based clinical staff?
Yes. Use QR kiosks in break zones, mobile text messages pulses between shifts, and embedded handover prompts for clinical staff. Keep surveys under 60 seconds and avoid peak clinical hours. These methods improve response rates without disrupting care delivery or requiring email access for participation.
5. What engagement questions should hospitals include for ICU staff?
ICU-specific engagement surveys should cover workload manageability, peer support during critical events, access to rest between cases, and leadership responsiveness to safety concerns. Avoid generic culture or career questions that miss the clinical reality driving engagement in high-acuity settings.
6. How often should hospitals survey different departments?
High-acuity units like the ICU and ED benefit from monthly or biweekly pulse surveys due to rapid workload changes. Lower-intensity departments, such as admin and support, can sustain quarterly cycles. Matching cadence to unit pressure improves data quality and reduces survey fatigue across teams.
7. How does nurse engagement affect patient outcomes in hospitals?
Lower nurse engagement is associated with higher rates of medication errors, increased patient falls, slower response to deteriorating patients, and elevated 30-day readmission rates. Measuring engagement at the unit level helps hospitals identify staffing and support gaps before outcomes are affected.
8. How do you measure engagement for travel nurses and float pool staff?
Travel nurses and float pool staff require a separate engagement track using mobile-first or QR-based surveys not tied to permanent department accounts. Questions should focus on onboarding, team integration, and access to support rather than long-term culture items irrelevant to assignments.






{kind=link}